The Brief: Deploy First Contact Physiotherapists in Primary Care
In mid-2022 the organisation I head up (Pure Physiotherapy) was approached by a primary care network (PCN) in England with a population of 56,000 patients across 5 GP practices, with a significant geographical spread. This meant that a physical hub model was not appropriate. In addition to this, they had two practices which were very limited in terms of physical space for First Contact Practitioners (FCPs) to work within. The task –
“create a First Contact Physiotherapy service which would enable rapid access, face-to-face provision, integration with trust/local pathways and offer education and advice to improve the patient journey with transparency”
The existing circumstances
The existing provision was a total of 2 full-time equivalents provided by a locum-type first contact practitioner model. They also had half of a full-time equivalent role from a local trust. As mentioned in a previous blog, a local model to first contact roles is difficult to support given their relatively recent introduction to primary care and the emerging governance around their roles.
I do believe there is a significant clinical risk as well as governance risks to practices with a locum-based First Contact Practitioner. This is outlined by the Health Education England road maps to practice documents, which identify key elements of competency and ongoing support needed to remain safe for both practitioner and patient.
The Primary Care Network contacted us was for a variety of issues which they haven’t been able to manage in the current structures utilisation of the service, this resulted in:
- Low utilisation (60-70%)
- DNA rate of 27%
- No patient feedback
- A reactive approach to provision
- Poor integration with local pathways (friction)
- Intermittent service, with annual leave and sickness concerns
Understanding the challenges
There was unusually low utilisation, especially given the population size and the number of First Contact Practitioners. Over the years in which we’ve been providing FCPs to primary care, we have concluded that approximately 1 full-time equivalent first contact physio will be able to competently match the demand of approximately 15,000 weighted header population per PCN.
So, with the population size of over 50,000, 2.5 full-time equivalents would seem appropriate, if not slightly under capacity. However, a low utilisation rate is a red flag and it would indicate something is not working particularly well within the first contact support service.
The second issue that was identified was a persistently high DNA rate. Generally speaking, we have found a national DNA rate of under 10% is not unusual for first contact services, which is in line with most primary care services. In some areas, this DNA rate is considerably lower and there are several factors which can influence this which I’ll discuss in a moment.
The existing provision created a DNA rate of 27%. This is an unacceptable level and certainly raises alarm bells about how the service was being described, and the value patients were putting on the service.
No patient feedback was being collected, nor was any feedback being provided to the Primary Care Network. This lack of feedback made it impossible to appropriately assess what needs to change in order to improve the service. I’m a firm believer in collecting clear transparent data in terms of outputs as well as regular patient feedback to assess the impact of the service, and also the patient’s perception and value they see in achieving first contact physiotherapy.
The other factor cited was a lack of proactive strategy for service delivery, which I believe was linked to the data (or lack thereof). There appeared to be a firefighting mentality to the way in which the first contact physiotherapy service was developing, rather than a planned and proactive approach.
The PCN described friction between partners, with the locum-based company providing two full equivalents, and the 0.5 equivalent from the local trust, which had led to difficulties in accessing local MSK pathways and imaging. Integration was also poor.
All in all, the existing service did not appear fit for purpose, and the PCN had rightly reached out to us for a review, and to see what could be done to improve the support their patients were receiving.
How to Maximise First Contact Physiotherapy
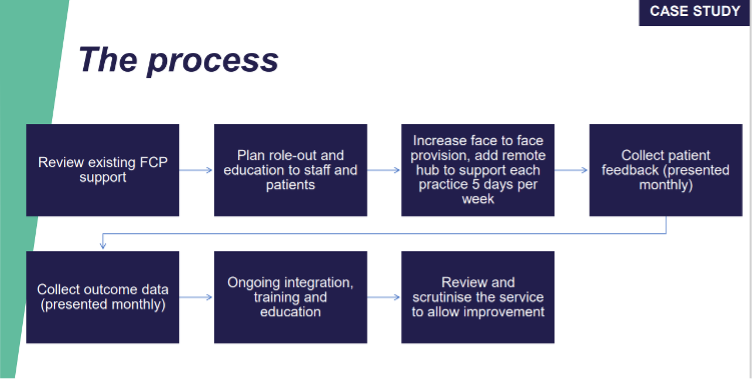
To improve the service we first reviewed the existing support, recognising that several factors were clearly incorrect in terms of data collection, integration with local pathways, communication with stakeholders, and education with the practices, reception team,, and clinical teams.
One of the key elements to a successful first contact service is the reception and administration team’s complete understanding of the value of the first contact service and how to get the maximum benefit from it. If this isn’t understood, it is very difficult for these teams to appropriately book patients in and describe the service as a valuable step for that patient.
The whole principle behind the NHS long-term plan was to enable patients to be seen by the appropriate practitioner in primary care rapidly. This principle is important if we are to understand and get the best from first contact roles. We developed a program of education for all staff and patients to improve their understanding and benefit from seeing a First Contact Practitioner.
It was relatively striking how little the reception teams understood first contact physio. This is not the reception team’s fault, and this is certainly not the first instance where we have encountered this challenge. This is a result of a lack of communication from the First Contact Practitioners or the structure that has put that in place. Ongoing training was subsequently put in place to ensure staff turnover or new staff coming into the reception role have received appropriate knowledge. All parties are then aware of the benefits of these different roles in primary care.
Collecting and understanding patient data
We also increased the face-to-face provision (where possible) and added a remote hub across the clinical system, which would allow each practice to access five days’ worth of the musculoskeletal first contact physiotherapy service. We immediately started collecting data for referral source, age demographics, waiting times, chronicity of each condition, and which surgery had referred them; alongside other key metrics.
Patient feedback was also collected and analysed on a weekly basis to see how we could improve and develop the service. Again, the patient feedback reinforced the need for education which was being developed alongside other changes.
Another important step was to reach out to the stakeholders, including community pathways, secondary care and local higher education institutes, as well as the local training hub. All of them were responsive and keen to see the situation improve, which we have typically found to be the case if primary care organisations proactively engage and are flexible in how we interact with existing pathways and healthcare systems.
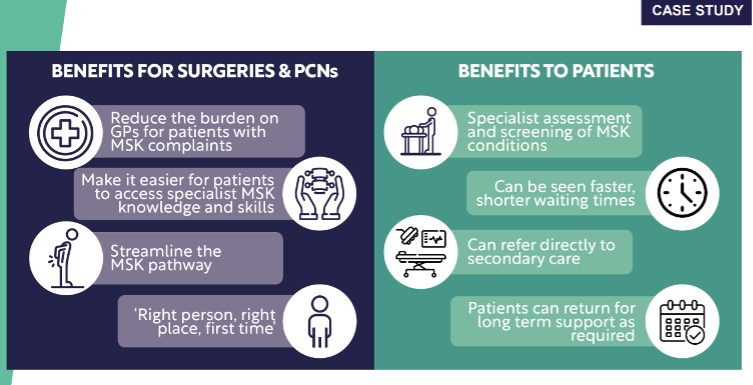
The benefits we saw within a relatively short space of time were, as you might expect, a reduction in pressure on GPs (in terms of the burden of patients with MSK complaints). Patients were able to access MSK specialist knowledge more rapidly. This was often same-day access, and the remote five-day-a-week hub made a huge impact on patient feedback. Especially the speed of access linked to the on-the-ground service, which in turn supported those who did require being seen face-to-face.
The integration with local MSK pathways also made a significant improvement to patient perception feedback because the waiting times were reduced, and we could manage expectations of patients seen in primary care moving to community and secondary care.
The outcomes of optimised first contact physiotherapy
We have now been supporting the Primary Care Network for over six months, and we have provided two full-time equivalent FCPs as was previously provided via the local model. We are also providing a fully supported service in a proactively managed way.
The local trust still provides 0.5 whole-time equivalents, however, we are working as one service and collaborating as one service within primary care. This has had huge benefits with the local pathway integration as well as improving the working conditions and enjoyment for all people involved.
Several key metrics of note are the image requests for ultrasounds, X-rays, and MRI scans, which have reduced from 12.6% to 2.1%. This represents an enormous reduction and an improvement in appropriate requests through to the radiology departments locally. We have also received positive feedback from these departments, because of this and the patients who require imaging have access with increased ease.
An audit on opioid repeat prescriptions for chronic pain patients in the PCN (for a sample group of 37 patients) has also seen a reduction of 7% in opioids for that patient cohort. This is something we are keen to continue to develop and will work with the clinical pharmacists and GPs within the PCN to continue to bring this figure down further.
Referrals to orthopaedics and secondary care have reduced to less than 1% of the patients we see, which is more in line with many of the first contact physio services running nationally. This improves the conversion rate of patients going to secondary care who actually require orthopaedic intervention.
The self-management rate of patients accessing the service is now at 69%, which again is roughly in line with our expectations for first contact physio services that are deployed well across England. This is supported by some of the information we’re able to send to patients post-consultation to facilitate positive behavioural change in terms of lifestyle, activity, and weight management – as well as improve their resilience to musculoskeletal issues going forward.
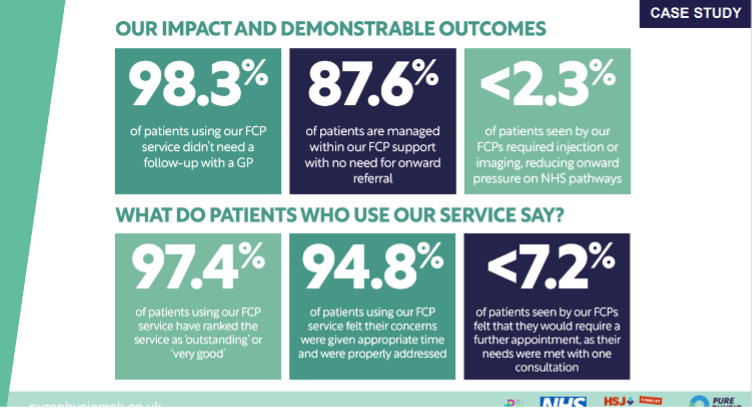
Patient feedback overall has been positive. The service has recorded over 97% of patients rating first contact physiotherapy consultations as outstanding or excellent. Over 94% of patients believe their concern was given appropriate time and addressed correctly within that one consultation. Only 7.2% of patients believe they would require more than one consultation to deal with their issues.
Key considerations for effective first contact physiotherapy
In conclusion, first contact physiotherapy can have a huge impact on up to 30% of the patients who attend primary care in England. It’s important to understand the definition of the role and its potential impact, whilst linking that to the local demographics and challenges faced within the operational area of the practice or PCN.
Ensuring that the implementation of a service is well understood with clear processes around diary management, annual leave cover, and training and development is critical. Recognising the importance of education to staff, particularly for reception teams, helps the service’s continual improvement through the use of patient feedback and data to inform and develop further.
If you would like to discuss any elements of first contact physiotherapy or the wider roles added I would be more than happy to please use the form below: